
Last week I visited India. I went as part of a leadership program organised by Wavelength. They brought together execs from companies such as the BBC and Jaguar Land Rover, charities such as the Prince’s Trust and fellow social entrepreneurs. There were 18 of us in total. We spent a whole week going deep inside what is arguably the world’s finest organisation – the Aravind Eye Care System.
When I explained that I was flying to India to visit an eye hospital, most people looked at me funny! I admit, it sounds a bit random! But it was a remarkable week, full of inspiration and learnings.
Aravind in a Nutshell
Aravind’s Beginnings
Aravind was founded in 1976 by a retired opthamologist (eye surgeon) called Dr. Venkataswamy (known as Dr. V). Despite developing rheumatoid arthritis at the age of 30, leaving him with crippled hands, he went on to become an eye surgeon. He personally performed over 100,000 eye surgeries over his career and retired at the age of 58. In his retirement, he decided to found an eye hospital to work towards eliminating needless blindness! So in 1976, he started an 11-bed hospital and used the profits it generated to build a multi-storey hospital, one floor at a time in Madurai, in southern India.
What Makes It the World’s Finest Organisation
Dr. V was inspired by the efficiency within McDonald’s restaurants and wanted to apply the same to his hospitals. So with meticulous detail, he fine-tuned every aspect of the running of his hospital to make it into an incredibly efficient machine. Today, surgeons perform five times more eye surgeries per day than the average eye surgeon in India. And they can perform an eye surgery for about 1/100th of the cost in the UK! They see less than 50% of the complications compared to the UK. And 25% the infection rate compared to the US!
Aravind is now a network of 7 large hospitals, a number of smaller hospitals and many small clinics in rural towns across southern India. They restored vision to ½ million people last year through cataract surgeries. That means that on average, someone’s vision is restored every minute! And they served over 4 million patients in total. They have a factory that manufactures intraocular lenses (the key component needed to treat cataracts). This has driven the price of these lenses down from $200 to $10, making cataract surgeries affordable for the poor.
Over 90% of their staff are young women recruited from rural villages who have no other employment opportunities. They provide free surgeries for people in rural villages who can’t afford them. And despite that, they are still wildly profitable (they made about $20M USD profit last year!) And they give all of their secrets away, including their software, to other eye hospitals around the world. They do this because they believe this is the best way to achieve their vision of eliminating needless blindness.
Convinced it might be the world’s finest organisation? 😉
Sunday: A Visit to an Eye Camp
On the first day of our trip (Sunday), we visited an eye camp. This was a gathering of people from the community with eye problems at the local school. Dr. V set up eye camps to help people in rural communities overcome the barriers they face accessing eye care.
We traveled for a couple of hours out of Madurai on a minibus to a rural village called Puliampatti. Once we turned up, we saw a long line of people queuing towards a table set up in the school courtyard. Once each person got to the front of the queue, they shared their details. These were written down by an Aravind employee on a piece of paper, which the patient kept with them.

The school classrooms were turned into six or seven different stations. Patients would start at the first station to have an initial examination. They would then be told to move on to the next appropriate station depending on their condition.

The Evolution of the Camp
One of the stations towards the end was a counselling service. Aravind introduced this after learning that only a small minority of people would actually attend their eye surgery appointment after being referred. When they looked into the reasons for this, they learnt that many people had fears about the surgery and chose not to attend. So they set up a counselling service. This gave patients who were referred for a surgery the opportunity to ask all of their questions and share their concerns. This significantly boosted the number of people who now attend their surgery.
Another reason people didn’t attend their surgery was because it was expensive to travel to the hospital and the longer they wait, the less likely they will carry through on their original intention. So Aravind now transport people to the hospital on the same day in a minibus. They provide this as a free service (along with free refreshments). This also had a dramatic effect on people having their surgeries. So not only do they offer free surgeries for people who can’t afford them, but they proactively break down the barriers stopping them from attending and even cover the cost of transport and refreshments!

The last station in the camp was where they actually produced glasses for the individuals who were prescribed them. They used to prescribe glasses at the camps, but the patient would then need to visit a store to buy them at a later stage. Many people didn’t do this for a variety of reasons. So they now produce the glasses at the camp. They have a special machine and a skilled operator who cuts and smooths a lens to fit within the frames that the patient has chosen. All within ten minutes!

Learning Through Data
It was clear to me that the evolution of this camp happened over many iterations, very similar to how great software products are built. They carefully measured the entire funnel of people moving through the different stages and figured out why certain drop-offs occurred (such as those not turning up to surgeries). They then made changes and measured further. Over a period of time, they found a highly efficient model for running very effective camps.
It’s incredible how data-focused they are. The staff who capture all of the data gather it together on the minibus home from the camp and type it up into the system as soon as they can. It is then analysed the next day or two by the team and senior staff and compared against benchmarks. For example, one of their many benchmarks is to make sure that over 70% of patients visiting the camps are over the age of 50 (to ensure those most likely needing treatment visit the camps). If any of these metrics are poor, they are investigated to learn why. But they don’t have a culture of individual blame. It’s all about the system and asking what they need to do within the system to make it more efficient.
Creating the Right Incentives
They also deeply think through incentives. For example, trust matters a lot to people, especially those living in rural villages. So what they find works well is to have a “community sponsor”. This is someone from the village who organises the camp and is responsible for getting people there. The sponsor also covers the costs of the running of the camp, either on their own or with the help of others. It is their way of giving back to their community. The community are far more likely to trust someone they know. So this drives up attendance and helps with costs too.
The Mix of Surgeries, Glasses & Medicines
And while they don’t charge for cataract surgeries, they do charge for glasses. And they don’t administer medicines at the camp. Why!?
Because they have learnt that people generally like taking the easiest options. Having medicine is the easiest for them. So when they administered medicines at the camp, people would prefer to take this option over having glasses or surgery. Even if it wasn’t best for them. By prescribing medicines, but not giving it to them there (they have to proactively visit a pharmacy at a later date to get this), this added enough friction to balance out the incentives so that more people accepted the best intervention for them.
The same goes for glasses. They come at a cost, but cataract surgeries are free. So this again balances out the incentives so that if the surgery is best for someone, they are more likely to accept this option. Moreover, people generally like “free things”. A pair of glasses is a materialistic thing. If given for free, most people want it even if it isn’t best for them. But cataract surgeries isn’t a “thing” that they own but a surgery done to them. Also, the system could be abused as people could get multiple pairs of glasses at subsequent eye camps, but couldn’t do this for eye surgeries. So they found that charging for glasses (they still only cost a few dollars) created the right incentives for people.
Monday: A Visit to the Hospital
On Monday, we visited the Aravind eye hospital in Madurai. We actually visited two hospitals – the “paid” hospital and the “free” hospital.
The Paid Hospital
We started in the paid hospital. As soon as a patient walks in through the front door of the hospital, they enter the system, which is even more finely tuned than the camp we visited. As most paying patients are literate, they are given a piece of paper to fill out.
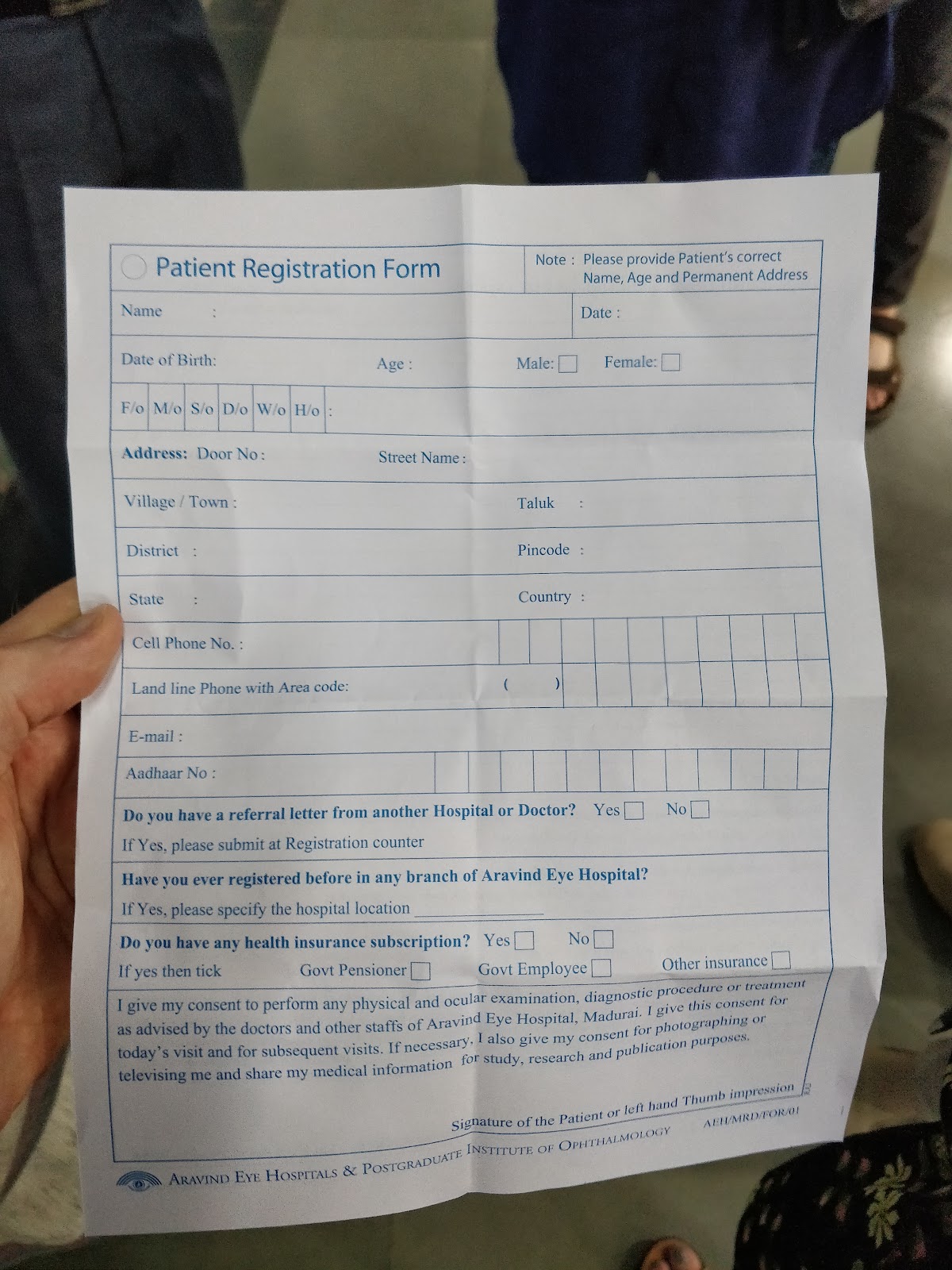
There are people in the lobby area to help them if needed. There are also computer terminals for people to type in their details directly if they prefer. For those that complete a paper form, they queue up and a typist will type their details into the computer system. But they have a monitor facing the person so they can verify that the details are accurate as they are typed in. It all sounds quite simple, but it’s actually finely tuned to ensure that people are registered efficiently and accurately.
I also noticed placards next to each department in the hospital that showed the objective of that department in relation to Aravind’s vision. This must be really motivating for the staff and probably keeps them really focused on their tasks.
I discovered at this point that they apply some pretty sophisticated data science to predict within 10% accuracy how many patients will walk in on any given day. They use historical data to predict this. They can then determine how many staff they need and at what capacity the staff can be expected to work that day so they can factor in whether to schedule other meetings.
Patient Movements & Tracking
Once a patient is registered, they wait in the area next door. But only for about 10 minutes! Imagine we had such consistently low waiting times in our hospitals in the UK! As the patients have vision problems, each patient that is called is given an assistant to escort them to where they need to go.
The hospital is arranged in a similar way to the eye camps in that there are different stations that a patient will move through. They will start with an examination, have access to a counselling service etc. The cataract surgeries themselves take place in a different building. Sometimes people would return the next day to have this done. But they would be given eye drops to administer themselves early that morning, which need administering a few hours before surgery. This ensures they can start operating as soon as the hospital opens and maximise their output of cataract surgeries.
They also tracked the number of minutes each patient has been in the system before being discharged. Any patient that has been in the system for over 90 minutes is flagged and efforts are made to find out why they have been waiting so long. There are screens all over the hospital showing the list of patients in each part and how long they have been waiting. There are also invitations for patients to leave feedback, which is carefully read by senior staff and acted on immediately.
The Free Hospital
We then went a few metres down the road to visit the free hospital.

Outside the hospital were a couple of hundred people sitting on the floor. This hospital didn’t have an indoor waiting area with seats. But they did have a canopy roof so people could wait in the shade. Everyone seemed very relaxed and happy. From what our tour guides said, they would probably feel very comfortable waiting in this way rather than inside in a seating area.

The registration took place outside too, but verbally instead of requiring each patient to complete a paper form. This is because most people who visit the free hospital are not literate. So they even optimised the registration process based on what works best for the patients who visit.
The way the hospital operated was otherwise very similar.
A Cross-Subsidy Model
The surgeries actually took place within this hospital and the patients recovered in a large room with beds side-by-side. Paying patients would have surgeries in a different location, but could access private, more comfortable rooms to recover. But both sets of patients had the same quality of treatment. They would both have intraocular lenses to replace their removed cataract lens. Even the surgeons would rotate between both sets of patients so they would all receive the same quality and the surgeons would maintain the same values of the organisation.
They compared this model to an airline. Whether you pay economy or first class, you both get the same quality of primary service. I.e. you both get transported to your destination by the same pilot with the same level of safety. But if you pay more, you have access to more comforts along the way. What’s interesting is the expectations of the patients. Those who pay would typically expect a private room to recover in because that better reflects their everyday reality and expectations. But a non-paying patient would typically be from a poorer, rural area. They may actually feel more uncomfortable being given a private recovery room. They would probably prefer to be in a larger room with other patients (in the same way that they were perfectly happy to wait on the floor outside). So not only does this model work, but it actually respects people’s preferences.
The paying patients cross-subsidise the free patients. It works because their operations are so efficient and they have such high volumes. Every day the network of hospitals perform 1,500 cataract surgeries. 500 of these are completely free for the patient. Another 250 are heavily subsidised. Despite this, they are still very profitable as an organisation!
Tuesday Morning: A Visit to a Primary Care Centre
On Tuesday morning we traveled almost an hour to a rural town where they had one of their many 73 primary care centres. These are small clinics that people in the local area can visit for an eye consultation.
The clinic had a small waiting area and a couple of rooms. In the main room was a computer terminal connected to the internet. Part of the consultation involved the patient talking via a video-link to a surgeon in the hospital. This enabled them to provide the same level of service as people received in the outpatients part of the hospital or at an eye camp. If surgery was required, they could simply book this at the clinic and travel to the hospital for surgery the next day.

Tuesday Afternoon: A Visit to the Factory
In the afternoon we visited Aurolab, the factory they founded in 1992 to manufacture intraocular lenses. Not only do they manufacture these lenses, but they now manufacture a whole array of other supplies to support their hospitals and others, such as needles, blades and pharmaceuticals.

What’s remarkable is that an organisation who founded a few eye hospitals decided one day to go into the business of manufacturing, with no prior experience! They did this to help them achieve their mission of eliminating needless blindness.
Intraocular Lenses and the Rationale for Building a Factory
So what are intraocular lenses? Well, a cataract surgery involves removing the natural lens within a person’s eye, which has developed a cataract (a clouding, causing it to be opaque and impairing the person’s vision). Once this lens is removed, a replacement lens is needed. This is called an intraocular lens and the surgery will involve putting this lens into their eye.
Back in 1992, intraocular lenses cost about $200. This was unaffordable for poor people. The alternative once a person’s cataract lens was removed was to give them thick, heavy glasses. But this was a much poorer intervention compared to inserting an intraocular lens into their eye. Not only would these glasses be heavy, but they could easily slip from their face (for example, as they work in the fields). This renders them effectively blind. So figuring out how to bring affordable intraocular lenses to everyone became part of their mission because they wanted everyone to have the same quality of treatment.
Fundamentally there was no reason why these lenses should cost $200. Dr. V was convinced he could manufacture them for about $10. And that’s what he did! They have been so successful that Aurolab now has 10% of the global market share for intraocular lenses. And they are no longer the cheapest because it has forced many other manufacturers to reduce their prices. The ripple effect here is remarkable! Not only can they provide affordable cataract surgeries of equal quality for everyone in their own hospitals, but now the cost of cataract surgeries across developing countries will have dropped due to the reduced price of these lenses! This is probably the single biggest driver of progress towards their mission of eliminating needless blindness!
The Factory Tour
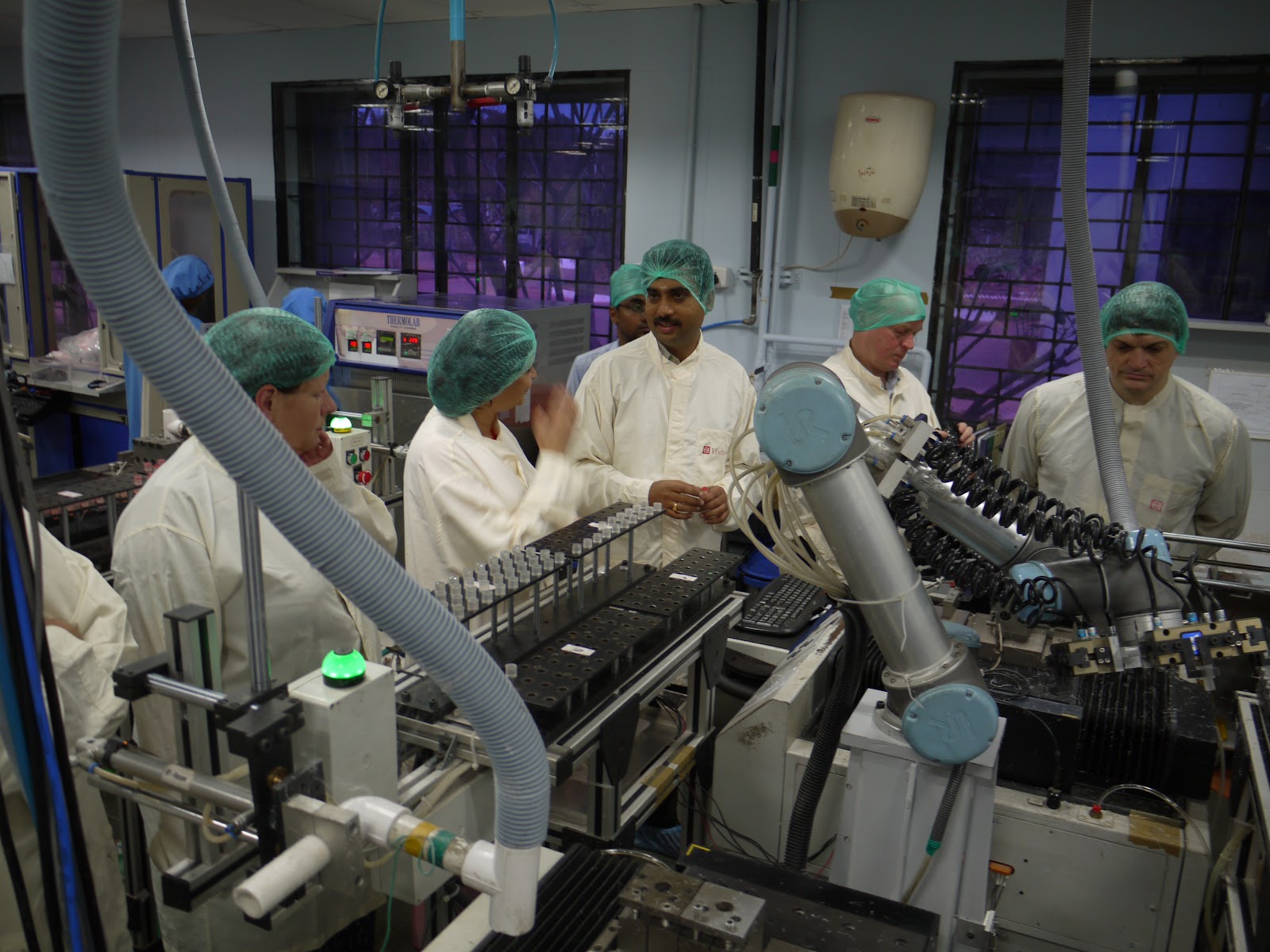
After an introductory talk, we split into two groups, put on the required clothing and entered the factory.

Factories amaze me! Manufacturing something physical from scratch at scale seems so complex. To see hundreds of packaged lenses coming off a conveyor belt boggles my mind. There are so many stages in their production, each with a variety of complex equipment and staff specialised in specific jobs. There was a room full of robotic arms that were moving things around, where the code that was used to program it was displayed on a screen and comprised hundreds of pages.
The amount of ingenuity, skill and knowledge that must have made up this factory (and other factories around the world) really is incredible. I guess it’s an evolutionary process, but to see the output and get exposure to its complexity was really interesting.

Final Interactions with Aravind’s Senior Leadership Team
Later on Tuesday afternoon we spent some time with Dr. V’s sister, Dr. Natchiar and other members of the senior leadership team at Aravind. Sadly Dr. V died in 2006. But it was very clear that his vision lives on and the progress of Aravind to eliminate needless blindness has continued and even accelerated. We took a walk with Dr. Natchiar. We learnt about her and Dr. V’s upbringing in a rural Indian village and the history of Aravind. We then had a final opportunity to share any remarks we had with the team and ask any final questions.

Dr. V successfully built a long-lasting, sustainable “operating system” at Aravind. This was a term they often used to describe it. The system is finely tuned and highly efficient. It doesn’t rely on any individual person, but is understood by every member and everyone plays a specific part in it. They have strong learning feedback loops and have a robust training program for new staff that enter. Despite Dr. V’s passing in 2006, the strength of this system is evident in how efficient it continues to be and how it continues to improve. It really is remarkable.

Wednesday & Thursday: A Visit to Aravind’s Biggest and Newest Hospital
Early on Wednesday morning we took a short flight from Madurai to Chennai (further north on the east coast of India). Aravind’s newest and largest hospital is built here.

The hospital is led by a man called Dr. Aravind. He is the nephew of Dr. V. He is trained as an opthamologist (as seems to be the case for almost everyone in the family!) and has worked for Aravind for over 25 years.
On arrival, we were warmly greeted by the team there.

Over the two days we were given a tour of the hospital. It was only operating at about 25% capacity, but they hope to increase this to 100% over the coming years. They have incorporated all the best practices from all of their hospitals to produce their most efficient design yet. They have an entirely modular design where each floor has five areas, all exactly the same. Each area serves about 300 patients per day, which they have determined to be the optimal number.
Witnessing an Eye Surgery
We also witnessed a few eye surgeries (we watched through a window next door to the operating theatre). The surgeon was Dr. Aravind’s wife and she took about 6-7 minutes to perform each surgery. The surgery involved extracting the patient’s natural lens that was clouded with a cataract and then inserting an intraocular lens.

The patient was awake throughout the procedure. As the surgeon was working on one surgery, the other staff would prepare the next patient on the other side of the room. So as soon as the surgery was complete, the surgeon would walk a couple of steps over and begin the next one.

We then had some really interesting sessions at the Chennai hospital. One session was with an artist in his 80s who was almost completely blind. He was a long-time friend of Aravind and shared his inspirational story with us. He kindly gave each of us a limited-edition print of one of his drawings.
We also had a session discussing Dr. Aravind’s latest project. He is collaborating with a nearby hospital to help people who need facial reconstruction. As people who need eye surgeries come for lots of different reasons, they cannot help people beyond eye interventions. But some patients require facial reconstruction in addition to eye surgery (such as victims of road traffic accidents). So they are working in collaboration with a local hospital who specialize in facial reconstruction to see if they can develop an efficient and affordable way to treat these people.
Wednesday Evening: Meeting other Indian Entrepreneurs
On Wednesday, Wavelength treated us to an evening of meeting some impressive local entrepreneurs. We met the founder of CavinKare, Mr. C.K.Ranganathan. He founded CavinKare in 1983 to supply products like shampoo to people in rural India. He has since expanded far beyond shampoo and has about 10% market share in India, competing against P&G and Unilever. We also met his son, who has grown a bakery empire in just three years. He operates a franchise of 77 bakeries in India, with plans to double in the next 12 months. And finally we met the CEO of a large media company in the midst of a turnaround in the wake of digital disruption.
Wrapping It All Up
On Thursday, we had a couple of sessions focused on purpose and trying to wrap up what we all learnt and took away from our week visiting Aravind.
We split into groups to try and summarise what we took away from it. Here’s what we produced …
Let me take a few moments though to share my own personal reflections on the organisation and my takeaways …
The Core of Aravind
At its core, Aravind is a finely tuned system. It works beautifully, sustains itself and continues to improve. Someone in the group described it as an “eye factory”. While that gets at the efficiency of the organisation, I think it’s more impressive than that. A factory (as I came to learn from visiting Aurolab) is a tightly controlled environment with no changing variables. But a hospital has an inflow of patients each day who have differing expectations, circumstances etc. Basically, they’re all human rather than components you get in a factory. And yet, they’ve built a system that can move people through it at incredible efficiency, giving them the highest quality treatment and keeping them happy. Not only have they done this, but they continue to improve, monitor and analyse every detail continuously and have managed to replicate it in multiple locations.
Values-Driven
And while they have a blueprint for doing all this, what’s most impressive is that it’s not just a playbook that people read. It’s actually embedded in the DNA of the organisation and by inference, everyone who works there. The way they train staff and the fact that those who run the hospitals have typically been there for two or three decades means that the way they work is so deeply embedded in all their staff and their culture.
What is most embedded though is their values. This was the one part that was emphasised the most and made them most distinctive. They are values driven. All of their values come from their vision to eliminate needless blindness. They are setup as a non-profit, so they have no competing profit-making agenda. And Dr. V instilled in everyone his own values, which Dr. Natchiar explained to me best:
- Live Simply
- Do what you do with all your heart
- And do it best
A Social Enterprise on Steroids
The other enormously impressive part of the organisation, which is actually secondary to their mission of eliminating needless blindness, is who they hire. Over 90% of their staff are women they hire directly from rural communities. These women would otherwise have little to no employment opportunities! And these women can often relate better to the rural patients as they have similar backgrounds and are happy to sit on the floor and talk to them.
The Scale
Over the past 8 months I’ve met a lot of social enterprises in London. They are all set up to provide some service. But the key differentiation is that they aim to hire marginalised individuals. Such as refugees, people coming out of prison, homeless people etc. But they all struggle to scale beyond hiring a handful of these people. They are still making a difference and I know it’s hard, but that just makes Aravind all the more impressive. Aravind has made phenomenal progress of eliminating needless blindness (with 12 million blind people in India and 39 million globally, they have performed over 4 million cataract surgeries to-date and are accelerating!). But in addition to this they also hire thousands of marginalised young women.
The Impact
Every year they hire about 200 18-year old women from rural areas. But they don’t stop there! They train them for two years and then employ them, typically for 3-4 years until they get married. They not only do this in the eye hospitals, but they also do this in the Aurolab factory too (the entire factory is run by these women). The women receive accommodation, food and an income. And they strongly encourage the women to save the majority of their income. So when they come to get married, the money they have saved can be used to help pay their dowments. This would otherwise often push families into debts they are unable to get out of. This then gives these women long-term opportunities for work, including flexibility to work in a more rural Aravind clinic.
These women then end up running the hospitals. Many of the operational senior staff at the Madurai hospitals were women that have been working in the hospital for 25+ years and originally came from rural villages.
It Could Literally Save Lives
One of the books I recently read, Poor Economics, talks about how the ratio of men to women in India is about 107:100. This means that women are less likely to survive. This could be because of selective abortions or being malnourished in the early years. It can also be due to not being breastfed for very long. This is because breastfeeding acts as a contraceptive and women sometimes want to try for another baby in order to have a boy before it is too late.
This all happens because women don’t have the same economic value in India as men. It is much easier for a man to get a job in India. In fact, women can be a drain on families as they often have to pay vast sums of money for their dowments when they get married. The amazing thing about the way Aravind is hiring these rural women is that it is making them economically valuable for their families. This could literally save women’s lives!
How Will This Inform My Journey?
Before I went on this trip, a lot of people asked me what I want to get out of it or how I expect it to help me. Honestly, I wasn’t exactly sure. It was one of those trips that didn’t have a very defined purpose. But I knew it would expose me to a lot and the learnings and context would likely justify it.
Having an inside tour of such an impressive organisation and having the chance to chat to 17 other people who had such diverse and impressive backgrounds meant that my brain neurons were firing a lot! I think the key value for this trip will be realized over the coming few years and beyond as I expect a lot of what I experienced will become relevant at different stages in my entrepreneurial journey in the future.
But here are a few specific things that are useful for me today …
Organisational Vision
Aravind has a great vision. We discussed what a great vision should be in one of our sessions. Mr. Thulasiraj (Aravind’s Executive Director) explained it well. He said the vision should be the one thing that unites the organisation and defines its purpose. It should be focused on outcomes and not process. And it’s the most fundamental, important part of Aravind and underpins everything else. So this is something I’ll be chewing on in the weeks to come as I ponder which direction I feel drawn to.
Hiring for Attitude
What struck me about how Aravind hire and also how the founder of CavinKare hires is that they focus primarily on attitude. I’ve not heard this focus in my previous companies. Previously, my primary focus on hiring is competence. But hiring for attitude is interesting. I can imagine that if you do this, you’re more likely to have a strong values-driven culture. So I’ll be sure to focus in on attitude in the future when I am hiring people and especially when I consider co-founders.
People at the Bottom of the Pyramid
One of our sessions was focused on the attitudes and expectations of people in rural villages and what Aravind has learned over the years as they try to serve these people better.
If my journey takes me towards serving people in developing countries, this will be useful context. One of my bigger ideas is to build an aid-based charity with tech baked into the tracking, logistics and donor experience. Imagine Amazon Prime for donors where you buy a malaria bed net for £1.60. You then track it in realtime from the factory to the recipient. And then you get a video from the family who received it, saying thank you. I have no idea if this vision is feasible, but that’s a big area I’ll be exploring in the months to come.
What Struck Me
So a few things struck me about what I learnt at Aravind about the people at the bottom of the pyramid:
- They demand respect. For example, banks in developing countries apparently don’t typically respect poor people. So when a poor person walks in, they might be interrogated as to why they are there. This lack of respect means that poor people don’t want to visit a bank, even if they have business there. Aravind took this on board and tries to respect all people equally. This helps ensure it doesn’t become a barrier to giving them eye care (and because it is the right thing to do and aligns with their values!). If I focus on delivering aid to developing countries in the future, this is certainly something I’ll factor in.
- They are very smart shoppers and investors. This is because their life depends on it! If we buy a shirt, but decide it doesn’t suit us or it’s the wrong size, we can just choose not to wear it. If a poor person in rural India buys a shirt and it’s not right, it could ruin them. This makes them very astute at shopping! So if I focus on delivering aid to people in developing countries in the future, I’ll try to understand the incentives that poor people have and their thinking when it comes to receiving free or subsidised aid.
- They seek trusted advice. This is probably because they lack information, so rely more on the trust of others. This is why it is important for Aravind to work through local partners and people living in communities to deliver their eye camps. And that’s why I’ll carefully consider working with local partners and people in communities if I work on delivering aid to people in developing countries.
All the Other Conscious and Unconscious Learnings!
And just the experience of being in India and being immersed in the culture and talking to the people there has taught me a tremendous amount. I won’t articulate my learnings and insights here, and frankly a lot of it is probably unconscious. But let me give you a flavour of why this experience has been so informative.
Immersed in India
Before the official Wavelength program began, I spent 2 days sightseeing as it was my first trip to India. So I visited a coastal town near Chennai called Mahabalipuram.
I visited one of the beaches where the tsunami hit in 2004. My tour guide, Sakthivel, told me stories of what he witnessed when he was at the beach that day. He said the joke of the day was that people were running to the mountains carrying their TVs on their heads. Sakthivel kindly invited me to his home to have lunch with him and his wife and I learnt all about how families in India live, what they value and the real estate market (or lack of!). Sakthivel’s brother took me on a boat ride to a temple that was mostly submerged under the ocean, 1km from the shore. But this temple became completely visible when the wave rescinded during the tsunami!
I sat under a tree next to a coconut stand chatting with the locals and learning about the economics of running a coconut business and its supply chain. I cycled through a village and observed how they access clean water and the facilities they had for sanitation. And then there was the overnight train trip I took, the many temples I visited (some of which were 2,500 years old!) and the many conversations I had with taxi and auto-rickshaw drivers.
So I’ve probably only captured 1% of my overall learnings in this blog post. And what I’ve learnt the most is the value of experience and actually spending time with people and learning from them. So whoever I serve in the future, I will try to spend some quality time with them and ask them a lot of questions to try to understand them as best I can.
Other Wavelength Attendees
And of course there were the other 17 attendees and the Wavelength staff who I spent many hours talking with. Everyone had such interesting backgrounds and I learnt so much from these conversations. I’m usually stuck in my tech bubble, only talking to people within my industry. So to have 5 intense days with such a wide range of people from a whole array of backgrounds was fascinating. And the value of the network you build over time usually yields so many benefits later on and this trip expanded my network in completely new ways.
So What’s Next For Me?
I’m Drawn to the Social Injustice that the Billion Poorest People Face
It’s been 7 weeks since my last blog post. Over Christmas I read one of the most inspiring books I’ve read for a long time – Thirst, by Charity: Water’s founder Scott Harrison. What struck me was that there are 663 million people in the world who still don’t have access to clean water. So children sometimes miss school because they have to walk for hours just to access clean water. And the water they then drink is dirty, taken from a stagnant pond with animal faeces in it. It’s disgusting.
I spent a day working with a homeless project in my home town in late December. I met about ten of their clients. They’re all having a hard time. But they do have access to clean water that comes out of taps. They have shelter (provided by the project). And they have access to benefits from the government. I feel that the social injustice of how the billion poorest live is so extreme relative to people in the UK, so I’m drawn to support them.
Big Idea 1: Tech-Enabled Aid-Based Charity
And that’s why I’ve been mulling over the idea of setting up an aid-based charity with tech baked into the foundations as I alluded to above. I’m flying to New York at the end of this month to spend some time with Scott Harrison to pick his brains on this.
But then there is the reality of doing this properly. If I deliver malaria bed nets at scale to villages in rural Africa, will there be an impact on the local economy (for example, what about the people who currently sell bed nets)? Or if they are so cheap, why don’t people already buy them? Are they a perceived need from people there and if not, will delivering them be really effective? I’m confident I could work through these and the many other complexities I would uncover. But it would take time and many trips. I would follow Ann Mei’s approach in her book, Lean Impact. Start small then iterate based on what I learn. But realistically that will take many months and possibly years before I scale, especially given my travel constraints with a young family.
Big Idea 2: Digital Platform to Help People Find Meaningful Work by Building Skills
So I’m also mulling over an area of focus in the UK too, which would be more feasible for me at this stage of life. The broad area that attracts me is helping people acquire the skills they need to find meaningful work. Employment feels like the silver-bullet of sustainably helping people. It gives people dignity, hope and independence. And if you invest in people’s skills, the impact could be sustainable. So I may actively explore this area further and see if technology could bring scalable impact here.
Beam, who I’m a trustee of, do this by crowdfunding the cost of training for homeless people to help get them back into work. The challenge here is scale as it relies on income from donors. This is such a competitive space with so many charities asking for money (although they plan to have their clients give back once they find work to fund future people in a more sustainable and scalable way). But could there be another approach? Maybe a digital platform that connects apprentices with experts with the right incentives to make it work?
In addition to these two big areas of exploration, I’ve now delivered two projects.
Project 1: Malaria Chatbot
I built a chatbot to raise money for the Against Malaria Foundation. Unfortunately the charity still haven’t got back to me. So I’m going to explore whether I can launch it independently of them and just send them a cheque with the money the bot raises. The US have a concept called a donor-advised fund that allows for-profit companies to raise money on behalf of charities. So I’ll explore whether there is an equivalent in the UK.
Project 2: Web App to Help Teachers Mark School Work in the Classroom
I completed the first version of second project before India. This is now being tested in a school in the UK. It is a web app that helps teachers mark papers in a classroom environment. Each student uses the web app on their smartphone or a shared iPad to take a photo of their completed work. They then see pairs of work from other students (not their own) and they have to make judgements over which they think is best. Each student does this a few times and the software stack ranks the results. This has a couple of benefits:
- It saves teachers hours in the evening marking the papers
- It helps students learn as they are exposed to many other pieces of work, in the context of the lesson and are forced to make a judgement on which they think is best. The best answer can then be shown at the end of the lesson to foster a classroom discussion on why this particular answer is best.
I’ll share more about this project in a separate blog post. But it’s going well and both the teachers and students seem to love it 😊
How Do I Pay the Bills?
Finally, I need to make some money! The two projects above could generate revenue, but they’d need to scale first (which takes time and is high risk). The two big areas above need quite a bit more time to flesh out before I can raise investment. So I’m also exploring paid consultancy work on projects that align with my personal mission of helping marginalised people with technology. This should help me learn and build more context too!
Wrapping Up this Blog Post …
So that’s where I’m at! Lots of moving parts, but I’m excited to try and launch the malaria chatbot and scale the education web app in the coming weeks!
Whatever comes next though for me, I’m thankful to have seen Aravind. For me it’s the world’s finest organisation. And if there is a finer one, I want to see it!
I wanted to end this post with a 12-minute video that one of the attendees on the trip, Maff, put together. It’ll give you a better flavour of what it was like than I’m able to do in words! …
Webmentions
[…] the first version in 7 working days (60 hours). I had some time pressure as I had an upcoming 10-day trip to India. If I shipped this first version before my trip, Ben and Dan would be able to test it while I was […]